

Introduction: Patients with acute myeloid leukemia (AML) are often treated with intensive induction chemotherapy to achieve complete remission (CR). Early response to standard anthracycline plus cytarabine induction (7+3) is assessed by a day 14 nadir bone marrow biopsy. The nadir marrow has limitations, though, including sampling issues and ambiguity as to whether blasts are leukemia cells vs. regenerating marrow. In prior studies, the predictive value for remission of the nadir marrow is only 67-84%. A more accurate predictor of residual disease (RD) would give clinicians an opportunity to modify therapy earlier. Positron emission tomography (PET/CT) with 3'-deoxy-3'-[18F]fluorothymidine (FLT) is a molecular imaging modality that can assess cellular proliferation in the bone marrow compartment. A prior single-institution pilot study showed a significant difference in the marrow FLT uptake between patients with AML who achieved CR and those who had RD after count recovery.
Methods: EAI141 was an ECOG-ACRIN-led, prospective, multi-center study designed to assess FLT PET/CT as a predictor of CR after AML induction. The primary objective was to evaluate the predictive value of post-treatment FLT PET/CT imaging for detecting RD, with the secondary objectives of evaluating the predictive value for detecting CR and estimating the sensitivity and specificity. Maximum standardized uptake value (SUVmax) of > 7 g/mL in total bone marrow compartment was chosen prospectively based on data from a pilot study as a marker for presence of leukemia cells at nadir. The predictive values, sensitivity, and specificity of the FLT PET/CT and the nadir bone marrow biopsy were calculated. Eligible subjects were 18 years or older with previously untreated AML who were to receive induction with 7+3. Subjects underwent a nadir marrow biopsy and an FLT PET/CT scan 10-17 days after starting induction, and prior to any re-induction if disease was noted on the nadir marrow. A recovery marrow was performed 28-35 days after initial treatment or re-induction to assess CR or RD. Subjects could undergo an optional pre-treatment scan. Relapse-free survival (RFS) and overall survival (OS) were additional clinical outcomes.
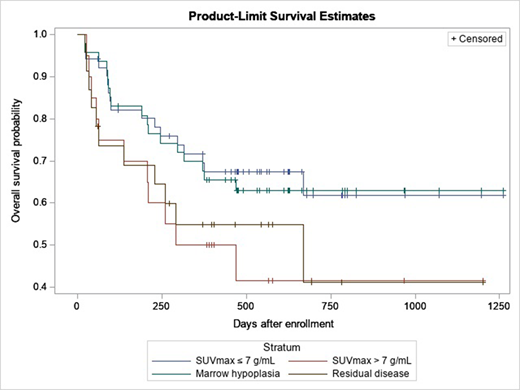
Results: 87 subjects from 9 centers were enrolled between 2016-2018, and 61 were considered evaluable. Reasons for being not evaluable included study ineligibility (n=3), no post-treatment scan (n=13), and no remission marrow (n=10). Median age was 58 years (range 21-73); 56% were men and 44% were women. CR was achieved in 56% (34/61). Treatment was a single induction course in 79% (48/61) and re-induction in 21% (13/61). Predictive value based on FLT PET/CT was 60% (9/15, 95% CI 32%-84%) for RD and 61% (28/46, 95% CI 45%-75%) for CR. Of patients who achieved CR, 28/34 had SUVmax ≤ 7 g/mL (sensitivity of 82%) and 9/27 of those who did not had high SUVmax > 7 g/mL (specificity 33%). Predictive value of an aplastic marrow was 59% (26/44) for CR and 56% (9/16) for RD. Of patients who achieved CR, 26/33 had marrow hypoplasia (sensitivity 79%) and 9/27 with RD had disease in the nadir marrow (specificity 33%). Significant heterogeneity of bone marrow compartment post treatment (SUVhetero ranging from 0.24 to 1.07) was observed in FLT-PET/CT scans. Heterogeneity of bone marrow compartment decreased about 50% from pre-treatment to post-treatment FLT PET/CT. OS for all participants, stratified by post-treatment FLT PET/CT response and nadir marrow results, are summarized in the Figure.
Conclusions: Although this study did not show significant advantage of FLT PET/CT compared to nadir marrow to predict RD or CR on the average, it did show signal heterogeneity in the study population that may be relevant to disease biology not appreciated by a single sampling site for the nadir or remission marrow. For example, in patients with false negative nadir biopsy, in approximately 20% of patients assessment with FLT PET/CT was correct, likely reflecting bone marrow heterogeneity and limitation of a single point sampling. Similarly, in almost 60% of patients with false positive nadir biopsy, FLT PET/CT assessment was correct.
Jeraj:AIQ Solutions: Current equity holder in private company. Kostakoglu:F. Hoffmann-La Roche: Consultancy. Strickland:KiTE: Consultancy; Kura: Consultancy; Astellas: Consultancy; Jazz: Consultancy; Pfizer: Consultancy; Novartis: Consultancy; Sunesis: Research Funding; ArcherDx: Consultancy; AbbVie: Consultancy. Uy:Daiichi Sankyo: Consultancy; Pfizer: Consultancy; Agios: Consultancy; Genentech: Consultancy; Jazz Pharmaceuticals: Consultancy; Astellas Pharma: Honoraria. Perlman:GE Healthcare: Research Funding; AIQ: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal